For many years, clinicians were taught to view the human foot as a simple triangle beneath the leg. Textbooks described it as a rigid lever with predictable axes and limited variability. Beginning in 1997, Dr Christopher Nester PhD at Salford University in England (he is currently at Keele University), and his international collaborators launched a research program that challenged these assumptions.
Across more than 165 peer reviewed publications since 1997, Nester has reshaped modern foot biomechanics. His work spans four major domains:
- In vivo foot and ankle biomechanics
- Evidence based foot orthoses.
- Footwear science and industry collaboration
- Clinical rehabilitation and technology
Although each of these areas has influenced modern podiatry, this blog focuses specifically on his in vivo foot and ankle biomechanics research. This is the body of work that directly challenged long standing clinical assumptions by mapping the precise, three-dimensional movement of internal foot bones during gait. This information from the Nestor bone pin studies has been useful discussing the joint motion available in the midfoot joints when teaching manual foot therapy and how a mid foot joint motion deficit can affect the forefoot.
I first met Chris Nester in 2006 at a Prescription Foot Orthotics Laboratory Association meeting in Chicago, where he presented his bone pin study results. The clarity and impact of that presentation were unforgettable. It was one of the few abstracts I kept from that conference. That moment shaped my understanding of foot mechanics and continues to influence how we teach biomechanics at painfreefeet.ca workshops.
When I was teaching biomechanics at the Michener Institute in 2009 to 2010, the bone pin motion data began to reshape the way I taught foot function. I decided to introduce the bone pin studies because they offered something I had not seen in the older motion data: a more direct picture of how the foot moved. I also introduced the contrast between the traditional two-axis midtarsal joint model and the emerging single-axis concept. The 2-axis model was referred to as a “theoretical convenience,” by Craig Payne and the phrase captures an important truth. Our biomechanical models are helpful frameworks, but they are still simplifications of a far more complex reality. For me, this period was when biomechanics became less about defending fixed doctrines and more about staying open to what better evidence was revealing.
These studies did not simply refine our understanding of the foot. They changed it completely.
Looking Beneath the Skin: How Nester’s Team Captured True Foot Motion
Traditional gait analysis uses skin mounted markers. The problem is straightforward. Skin moves independently of the bones, which creates large measurement errors.
To reveal the true behaviour of the foot, Nester’s group used two high precision methods.
1. Invasive In Vivo Bone Pin Studies
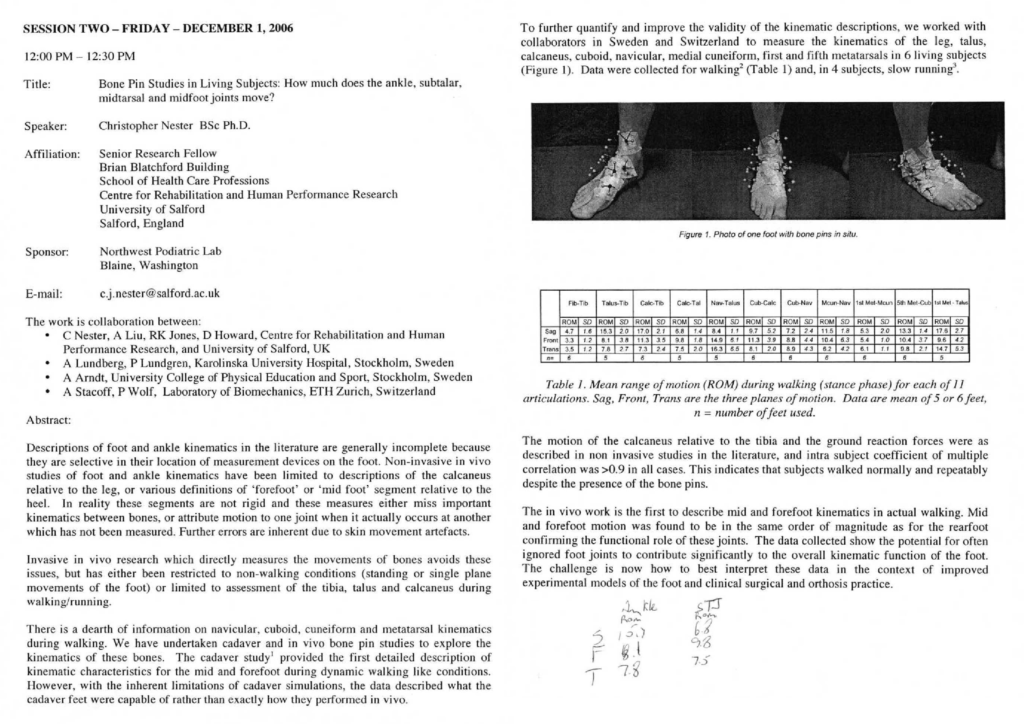
Reflective markers were attached to intracortical bone pins drilled directly into the bones of living volunteers. This allowed researchers to track actual bone motion during walking.
2. Dynamic Cadaver Simulators
Cadaver feet were fitted with motors that applied tendon tension to mimic real muscle pull. This made it possible to observe deep tarsal motion that cannot be seen clinically or captured by surface markers.
These methods produced the most accurate foot movement data available at the time, and the results were quite different from traditional models.
A Note on Sample Size and Generalisability
The authors acknowledged that their small sample sizes, typically four to six volunteers for bone pin studies and thirteen specimens for cadaver models, limit generalisability. Nester (2009) noted that although the data are not representative of the wider population, they remain essential because they directly refute long standing biomechanical assumptions and show that high inter subject variation is normal in healthy feet.
The small participant pools were an unavoidable consequence of the invasive procedures. To address this, the researchers focused on identifying consistent kinematic patterns that appeared across most subjects, allowing them to define functional units based on shared behaviours. They argued that the accuracy of these gold standard measurements, which capture true bone motion without skin movement errors, outweighs the statistical limitations.
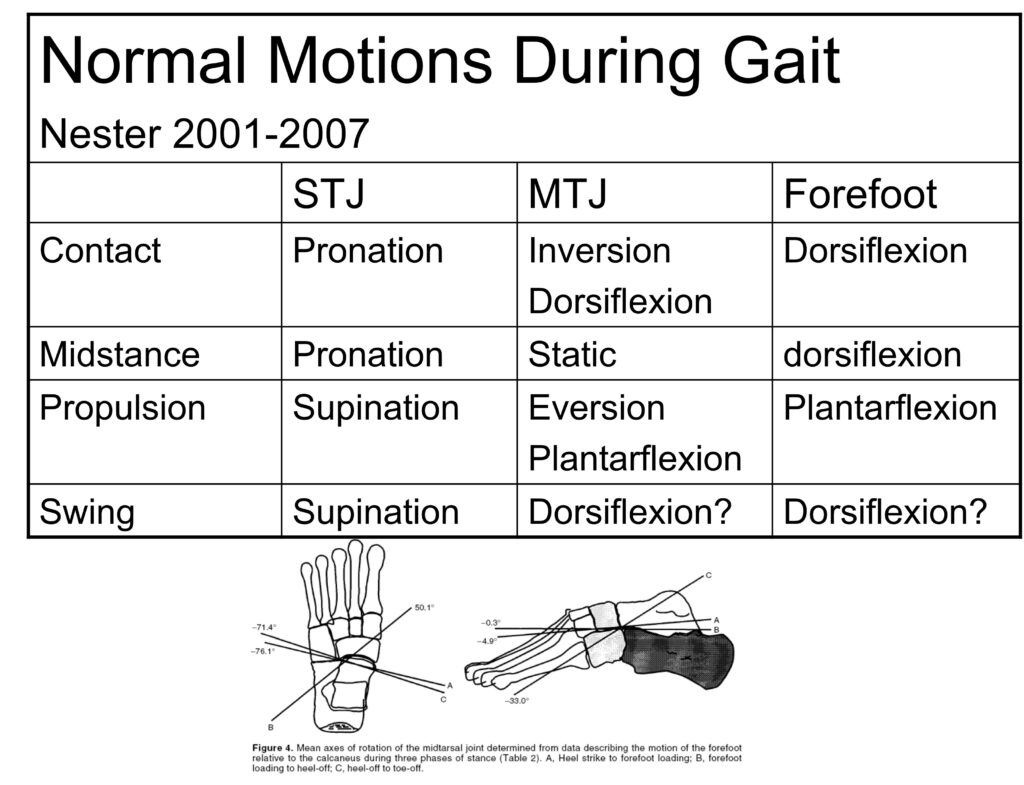
The Ankle: Not a Hinge but a Multiaxial Joint
For decades, the ankle joint was described as a simple hinge that moved only up and down. Nester’s early work showed that this description was incorrect.
- The ankle produces meaningful transverse and frontal plane motion, often greater than 15 degrees.
- In many individuals, the ankle contributes more transverse rotation than the subtalar joint.
- The ankle therefore shares the torque converting role that was traditionally assigned only to the rearfoot.
This finding requires a rethinking of ankle mobility, compensation patterns, and orthotic design.
The Midtarsal Joint: A Changing Axis, Not Two Fixed Ones
The classic midtarsal joint model relied on two fixed axes: longitudinal and oblique. Nester’s bone pin studies demonstrated that this model does not match real foot behaviour.
Instead:
- The midtarsal joint operates around a single instantaneous axis that changes orientation throughout gait.
- The navicular and cuboid move as a functional unit, rotating in the same direction at the same time.
This reframes the midfoot as a dynamic and adaptable structure rather than a rigid block.
The Midfoot and Forefoot: Far More Mobile Than Expected
One of the most important insights from the 1997 to 2009 research period was the high mobility of joints distal to the rearfoot.
Medial Column Mobility
The navicular, cuneiforms, and first metatarsal collectively produce approximately 29 degrees of sagittal motion. This is like the combined motion of the ankle and subtalar joints.
Lateral Column Lowering
The fourth and fifth metatarsals are significantly more mobile than the medial metatarsals. This contributes to a functional lowering of the lateral arch during stance.
Cuneiform Navicular Motion
This joint, once thought to be rigid, provides 10 to 11 degrees of movement.
These findings challenge the long-held belief that the midfoot is inherently stiff.
Walking and Running: The Stiffness Paradox
Bone pin studies revealed a surprising pattern.
- Most intrinsic foot joints move less during slow running than during walking.
- The ankle moves more to absorb impact, but the rest of the foot becomes stiffer.
- This stiffness is due to increased muscular and external stabilizing forces.
This suggests that stiffness is not necessarily a sign of dysfunction. It can be a functional strategy.
Clinical Implications: A More Individualised Approach
The research published between 1997 and 2009 reshaped clinical practice in several important ways.
1. Orthoses Must Support the Midfoot, Not Only the Heel
Because the midfoot is highly mobile, heel wedges alone are often insufficient. Effective orthoses should provide total contact support across the rearfoot and midfoot.
2. Lateral Wedges for Knee Osteoarthritis
Laterally wedged insoles reposition the ankle and subtalar joints. This reduces the varus moment in medial knee osteoarthritis and can be more effective than knee braces.
3. There Is No Single Ideal Foot Type
Nester’s early work rejects the idea of a single normal or Root foot. Asymptomatic individuals use a wide range of kinematic strategies to walk.
Variation is normal. Variation is healthy.
Conclusion: The Foot as a Dynamic Gearbox
Nester’s first decade of research shows that the foot is not a rigid lever. It is a dynamic and adaptable gearbox made of interdependent joints that constantly reconfigure themselves to meet the demands of movement.
For clinicians, the message is clear.
- Move beyond universal mechanical ideals.
- Recognize that joint axes shift and mobility varies.
- Treat each foot as an individual system with its own unique solutions.
This foundational work continues to influence modern biomechanics and remains essential reading for anyone who wants to understand how the foot truly functions.
From the manual foot therapy perspective, Drs Hiss and Tikker both recognized that midfoot joints needed to flow freely. And comfort varies with function.
References
- Arndt, A., Wolf, P., Liu, A., Nester, C., Stacoff, A., Jones, R., Lundgren, P., and Lundberg, A. (2007). Differences in ranges of motion in intrinsic foot joints during walking and running. Journal of Biomechanics, 40(S2), S94.
- Arndt, A., Wolf, P., Liu, A., Nester, C., Stacoff, A., Jones, R., Lundgren, P., and Lundberg, A. (2007). Intrinsic foot kinematics measured in vivo during the stance phase of slow running. Journal of Biomechanics, 40(12), 2672–2678.
- Hall, C., and Nester, C. J. (2004). Sagittal plane compensations for artificially induced limitation of the first metatarsophalangeal joint: A preliminary study. Journal of the American Podiatric Medical Association, 94(3), 269–274.
- Lundgren, P., Nester, C., Liu, A., Arndt, A., R. Jones, Stacoff, A., Wolf, P., and Lundberg, A. (2008). Invasive in vivo measurement of rear-, mid- and forefoot motion during walking. Gait & Posture, 28(1), 93–100.
- Nester, C. (2006, December). Bone Pin Studies in Living Subjects: How much does the ankle, subtalar, midtarsal and midfoot joints move? Presented at the Prescription Foot Orthotic Laboratory Association (PFOLA) Conference, Chicago.
- Nester, C. J. (1997). Rearfoot complex: a review of its interdependent components, axis orientation and functional model. The Foot, 7(2), 86–96.
- Nester, C. J. (1998). Review of literature on the axis of rotation at the sub talar joint. The Foot, 8(3), 111–118.
- Nester, C. J., Findlow, A., and Bowker, P. (2001). Scientific approach to the axis of rotation at the midtarsal joint. Journal of the American Podiatric Medical Association, 91(2), 68–73.
- Nester, C. (2006, December). Treatment of Medial Knee Osteoarthritis: Biomechanical Effects of Valgus Insole Wedges versus Knee Braces. Presented at the Prescription Foot Orthotic Laboratory Association (PFOLA) Conference, Chicago.
- Nester, C. J., and Findlow, A. H. (2006). Clinical and experimental models of the midtarsal joint: Proposed terms of reference and associated terminology. Journal of the American Podiatric Medical Association, 96(1), 24–31.
- Nester, C., Jones, R. K., Liu, A., Howard, D., Lundberg, A., Arndt, A., Lundgren, P., Stacoff, A., and Wolf, P. (2007). Foot kinematics during walking measured using bone and surface mounted markers. Journal of Biomechanics, 40(15), 3412–3423.
- Nester, C. J., Liu, A. M., Ward, E., Howard, D., Cocheba, J., Derrick, T., and Patterson, P. (2007). In vitro study of foot kinematics using a dynamic walking cadaver model. Journal of Biomechanics, 40(9), 1927–1937.
- Nester, C., Bowker, P., and Bowden, P. (2002). Kinematics of the midtarsal joint during standing leg rotation. Journal of the American Podiatric Medical Association, 92(2), 77–81.
- Nester, C. J. (2009). Lessons from dynamic cadaver and invasive bone pin studies: do we know how the foot really moves during gait? Journal of Foot and Ankle Research, 2(1), 18.
- Nester, C., Findlow, A., Liu, A., Ward, E., and Cocheba, J. (2005, October). Redefining Biomechanics of the Foot and Ankle. Podiatry Today, 18(10).
- Nester, C. J., Findlow, A. F., Bowker, P., and Bowden, P. D. (2003). Transverse plane motion at the ankle joint. Foot & Ankle International, 24(2), 164–168.
- Wolf, P., Stacoff, A., Liu, A., Nester, C., Arndt, A., Lundberg, A., and Stuessi, E. (2008). Functional units of the human foot. Gait & Posture, 28(3), 434–441.